

Shoulder Impingement

Shoulder impingement is a common term thrown around these days but for the most part it’s pretty useless diagnosis, but a great billing code.

The challenge of this diagnosis is that it doesn’t describe a source, it describes a mechanism. The tissues in the shoulder always “impinge,” especially at end range (true for most joints). All the tests we do just take you to an end range and apply resistance. If something is irritated, it will likely recreate your pain.
There are 2 types of impingment
External (primary and secondary)
Internal
External Impingement
Since “impingement” is nonspecific, the new term is Subacromial Pain Syndrome. Something (bursa/tendon) under (sub) the acromion is getting compressed by the acromion or coracoacromial ligament. Since it is irritated, it hurts when it gets smooshed.
This compression ALWAYS occurs, even in pain free shoulders. That red spot is the subacromial space.

Recall 2 types
Primary External Impingement
Primary is structural. A common thing to blame is acromion type. You can see in the not realistic cartoon sketch below there are 3 types. Notice Type III has a scary looking hook making the space more narrow, making it easier to compress the tissues.
It looks scary too since it’s basically a hook straight out of a horror movie slashing your rotator cuff. Rest assured that is NOT happening.

Acromion type being an issue is debated for a few reason. One, there’s no good way to measure it since humans don’t look like cartoon drawings. Imagining isn’t good enough, and actual scapula position (which can vary person to person or standing vs. sitting vs laying) can change the angle.
Oh yeah, and the margin of error of the measurement device can be larger than the recorded differences of the types.
Two, cuff tear severity is not related to acromion type. You can have a massive cuff tear with Type I, or a small tear with Type III (on the off chance you can ACTUALLY tell the acromion type!) This is true with progression too, type does not mean slower or faster degenerative progression.
Third and final, it doesn’t appear that you have a choice since it’s possible your type is predetermined. They did a study where they looked at a bunch of shoulders and saw a variety of types, so they thought it changed over time.
Then they did a study where they looked at a bunch of the same shoulders over 3 years and none of them changed. It’s possible 3 years isn’t long enough.
Basically we don’t know shit.
It’s likely all related to overall rotator cuff muscle quality. So, you know, you should exercise.
Secondary External Impingement
Secondary is related to impaired strength and mechanics of the cuff muscles and the scapula muscles. So, you know, you should exercise.
Both primary and secondary likely have strength and ROM deficits, secondary won’t have the (as much?) associated structural stuff. Makes sense since Primary is the most common and usually affects older (> 40yo) folks. The longer you are alive, the greater chance to get all these things. Another argument for tissue quality. So, you know, you should exercise.

Internal Impingement
This is impingement in the back of the shoulder and it is common in throwers, i.e., baseball pitchers. Makes sense right, throwing a baseball really hard requires a lot of shoulder ER (range of motion BELOW the table), so people that throw baseballs really hard will have a lot of shoulder ER.
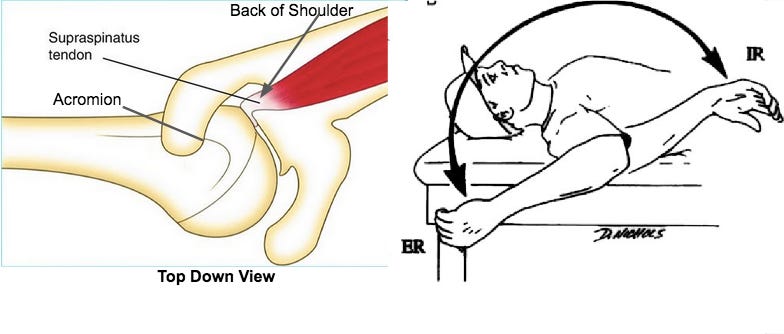
There can be associated limitations (stiffness) into overhead and internal rotation, and the front of the shoulder can be “loose” to allow that much extra ER rom. This can later lead to a cuff tear or labrum issues.
Pain with internal impingement is usually felt in the back of the shoulder (left picture) during things like the late cocking phase of throwing or putting on a jacket.
I’ve currently treating a 17 yo female in the band and a 43 yo male pilot (yes, he is dangerous) that have ROM just like the baseball player picture above. The female’s symptoms are not consistent with internal impingement.
Diagnosing Impingement
There are bunch of special tests to assess your shoulder and help diagnosis which type of impingement you have, but they aren’t very specific. Basically you say “my shoulder hurts when I do xyz,” then I perform tests that closely mimic xyz, at which point you say “OUCH,” making the test positive. I perform the test expecting it to be positive.
Your history (location of pain, activities that hurt, recent changes in activity) are the most important since they will dictate which tests I use to confirm what I think is wrong with you, if that even matters.

Treatments for each all involve the same thing - treat the impairments. Examples of impairments include:
Pain - oscillations, soft tissue work, isometrics
ROM - stretching/eccentrics
Strength - resistance training
These are all done in a manner that are within what you can tolerate do we don’t irritate whatever is irritated, then slowly load them up again to improve their tolerance.
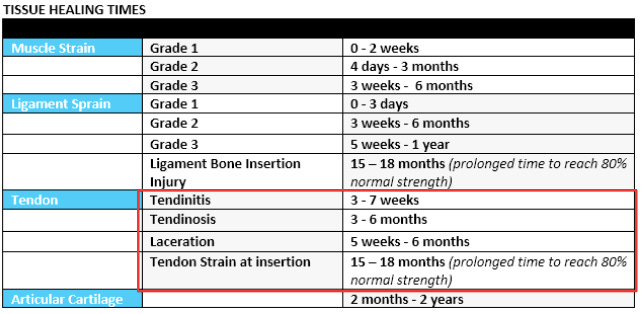
Healing is the hard part, especially since it usually involves tendons. They don’t have as good of a blood supply as muscles, so it can take longer. Standard for any soft tissue injury is the default 3-7 weeks with tendinitis, and more chronic type stuff like tendinosis can take 3-6 MONTHS!!
You can read a little more about stages of tendon healing from a previous substack (link).
One thing to keep in mind is that pain is not a good indicator of what’s going on in the tissues. You can have no pain but the tendon has low tolerance, so as soon as you start pushing the intensity (heavier weight, faster speed, etc), the pain can come back if you exceed your tolerance.
Summary
That wraps up the basics on shoulder impingement. It is not a great diagnosis since it just describes what is happening, not what tissue is involved. Often it’s related to overloading some tissues beyond what it’s capable of tolerating. Healing can be slow, so the goal is to treat the impairments (pain, ROM, strength) as things heal. Over time, your tolerance will improve.