


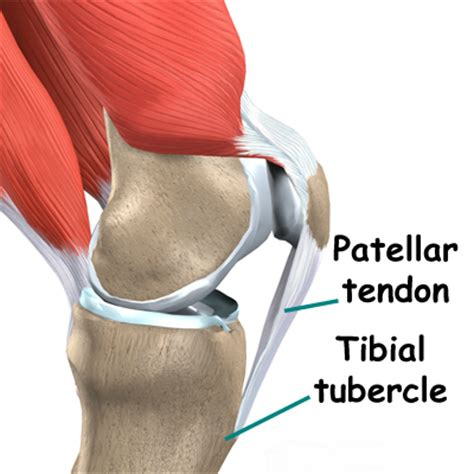
Using Isometrics to treat Patella Tendinopathy

This is the rationale and sample template of the isometrics protocols I use to treat tendinopathy. I’ve had some success treating patella and Achilles tendon issues in terms of pain management and function. Let’s dig in.
Tendon Pathophysiology
Pathophysiology is a fancy word for the changes to the tendon caused by disease or injury. For our purposes, we will be talking about injury.
Generally speaking, a tendon will go through phases in response to loading. When a tendon is excessively loaded, it will become “reactive,” or softens. Examples are a young person running 5 miles after doing nothing for 6 months, or an old person WALKING 5 miles after doing nothing for 3 months. This is your typical “overuse injury.”
There’s more technical things going on in the actual tendon substance, but I’m not going to pretend I’m some tendonologist (not a thing) and go into an in depth analysis. As the tendon repairs/adapts, it becomes thicker/stiffer to be better prepared for next time (just like muscles).
This is a transition phase, and the tendon can revert back to its normal state. Issues arise if you continue to excessively overload the tendon beyond what it can tolerate. Worth noting that loading tolerance is DECREASED in this phase, so you have to do less, or you will progress to a state of tendon “dysrepair.” Ultimately you may progress to the “degenerative” stage, which has a poor prognosis for recovery.
Why Isometrics?
Eccentrics are often used for tendinopathy since you can handle more weight - you can lower into a squat with MORE weight than you can come up with. The drawback to eccentrics is a phenomenon called stress shielding. The stronger parts of the tendon “shield” the weaker areas from stress. With eccentrics, the idea is to “treat the donut, not the hole.” As a result, the strong part gets stronger but shields the weaker part more, thus making the weak part weaker.

New thinking utilizes the phenomenon of stress relaxation, a fundamental property of tissues similar to tendons (viscoelastic, if you care). By applying a load to the tendon WITHOUT changing its length (isometric contraction), over time, the tendon relaxes/gets less stiff, and the stress can be spread throughout the entire tendon. This is thought to restore tendon health. Pretty neat-o.
Additional Benefit
Isometrics can also be good for pain relief, especially immediately after you complete the set. The HOW isn’t understood, and depending on what your issue is, any type of loading (isotonic or isometric) can be beneficial for pain relief. If isometrics don’t change pain, its possible 1) the tendon isn’t your issue or 2) you’re tendon is too sensitive/irritable to ANY load.
How To:
Simply just start with 1-2 exercises, 2x/week. There is a top end, but it would depend on all the activities you are doing. The above prescription was used on an NBA player, so it was low volume since it was during the season. The case report is here:
https://t.co/gX02VSmMFA
Below is a sample program, starting at 3 sets of :10 seconds, ultimately getting to 2 x :30 seconds every 4 weeks. The same loading is done on each exercise. Exercise selection is based on ability to load more than anything else since the goal is just to progressively load the tendon. It’s easier to hold mid range on a leg press than a back squat.
The isometric needs to be held at MID range. So for leg extension, push the weight all the way up, come back half way, move one leg out of the way. Hold it for the desired time, repeat with the other leg. Systematically increase the weight.

This case report also used gelatin in conjunction with the loading program. The player had 15g of gelatin mixed in 16 oz of orange juice (225mg Vit C) 1 hour before the session. This timing was to enhance nutrient delivery. Feel free to look up the effects of gelatin on tissue healing.
Summary
This can easily be adapted to the patella or Achilles tendon. For the Achilles, you can do heel raises with the knee bent and straight. It would take some experimentation for other tendons that are commonly involved, like the lateral elbow or the biceps tendon.
This is “easier” but it is still volume, so you may not be able to just add this in, you may have to remove items. Your symptoms and injury history will dictate.